Thumb Sprains
What are thumb sprains?
A sprain is an injury to a ligament. Ligaments are the connective tissues that connect bones to bones across a joint. The most common thumb sprain involves the collateral ligaments of the Metacarpophalangeal (MCP) joint.
How do thumb sprains occur?
These types of injuries are common in sports and falls on to an outstretched hand. The thumb is jammed into another player, the ground, or the ball. The thumb may be bent in an extreme position, causing a sprain. The thumb will usually swell and may show bruising. It is usually very painful to move.
What are the most common types of thumb sprains?
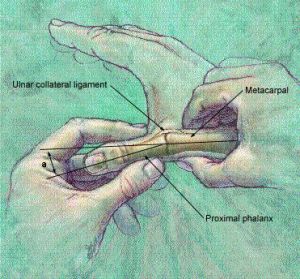
The most common ligament to be injured in the thumb is the ulnar collateral ligament (see Figure 1). Injury to this ligament is sometimes called “skier’s thumb” because it is a common skiing injury. It occurs when the skier falls and the pole acts as a fulcrum in the hand to bend the thumb in an extreme position. This ligament may also be injured by jamming the thumb on the ground when falling or by jamming the thumb on a ball or other player. The radial collateral ligament may also be injured. The radial ligament is much less commonly injured than the ulnar collateral ligament (see Figure 1). For many years an injury to the ulnar collateral ligament of the thumb MCP joint has also been called "gamekeepers thumb" after the chronic injury to that ligament suffered by a gamekeeper reportedly this phrase has been attributed to
What are some signs that this injury may have occurred?
Characteristic signs include pain, swelling, and bruising around the thumb , and especially over the MCP joint of the thumb. The patient will often manifest a weakened ability to grasp objects or perform such tasks as tying shoes and tearing a piece of paper. Other complaints include intense pain experienced upon catching the thumb on an object, such as when reaching into a pants pocket.
How are thumb sprains treated?
X-rays are usually taken to make sure the bones of the thumb and hand are not fractured. Sometimes "stress" X-rays are also used. Your doctor will then examine the thumb to determine whether the ligament is torn. If the ligament is partially torn, it is usually treated in a cast or splint. Radial collateral ligament injuries are frequently treated this way as well. The end of a completely torn ulnar collateral ligament often gets trapped behind a tendon. This "trapping" of the ligament in the edge of the aponeurosis is known as a Stener Lesion. Complete ulnar collateral ligament tears are most commonly treated with surgery to repair the ligament. The presence or absence of a Stener Lesion is at times used to determine whether surgery is needed but typically complete lesions or ligament tears require surgery. Sometimes the remaining ligament tissue is of poor quality and the ligament must be reconstructed with a tendon or ligament graft. A partial strain that does not require referral can be treated with either a thumb spica cast or a gamekeeper's thumb splint for four to six weeks. Active range of motion exercise is started at three to four weeks, with gradual return to full activity.
Chronic Injuries
The term “chronic” refers to an old injury of greater than one or two months duration. In this case, the joint may be unstable with symptoms of pain, especially with pinching. The joint may feel loose and strength may be decreased. These injuries may be treated by reconstruction of the ligament, or joint fusion if arthritis is present. Untreated tears can cause disabling instability of the hand, since the ulnar collateral ligament stabilizes the first MCP joint when the thumb is adducted against the index and middle fingers when gripping objects. Reconstruction typically involves taking a small piece of tendon tissue from the wrist to be placed into the thumb joint. At times radial sided tears undergo conservative treatment even in chronic situations. Ulnar sided tears typically do not do as well with intial conservative treatment If conservative treatment fails surgery may be indicated
Associated Injuries
On occasion, fractures may occur along with thumb sprains. These may require additional surgery with repair using metal pins, screws, or plates. Cartilage damage may occur as well which does not show up on x-ray. This occasionally results in long-term pain and eventual arthritis. Some patients may benefit from cortisone injections or eventual surgery.
What happens and what should I expect after surgery?
A cast is placed on your thumb, wrist and forearm for approximately 4 weeks. Your thumb tip and your fingers are left free. After the cast is removed, the pin that holds your joint in place is typically removed in the office. You then go to hand therapy and are fitted for a removable splint that is very similar in size and shape to your cast. However you can remove this splint for exercises and range of motion. At first you will remove the splint under the supervision of the therapist. As you progress you will be instructed by the therapist to remove the splint in controlled situations for exercise and use. It still takes another month at least before you can use your hand without limits or splinting. Some take longer, others go faster, but overall you have to consider it to be a 2 -3 month process.
Failure to wear a cast, and then a splint and deciding not to go to therapy can limit or compromise your result. In general some loss of motion of the thumb occurs but the goal is to have a stable thumb joint for activity.

|

|

|
Figure 1: The ulnar collateral ligament (UCL) and the radial collateral ligament (RCL) help stabilize the thumb.(right) Abduction and extension and UCL injury
|

|
Figure 2: (left) Stress testing of the affected thumb is often used in comparison to the normal thumb. Sometimes a nerve block or local anesthetic is injected in to the area to facilitate the exam. (right) The thumb adductor aponeurosis is interposed between the ruptured distal ligament end and the bone surface in this diagram of a Stener lesion.
parts taken from ASSH © 2006 American Society for Surgery of the Hand. Developed by the ASSH Public Education Committee,
with additional information and figures adapted from http://www.aafp.org/afp/980115ap/ballas.html and http://innervate.exblog.jp/10112052/.
More Reading
Clinical Testing of Ulnar Collateral Ligament Injuries of the Thumb
A. K. MALIK T. MORRIS D. CHOU E. SORENE, E. TAYLOR
From the Department of Hand Surgery, University College London Hospital, London, UK
The diagnosis of complete tears of the ulnar collateral ligament of the thumb metacarpophalangeal (MP) joint depends on demonstration of excessive laxity of the ligament, but there is controversy on whether laxity greater than a certain cut-off value or laxity greater than the opposite thumb is the criterion for diagnosis. We examined 200 thumbs of 100 normal individuals in extension and in 30° of flexion. In 34% of subjects there was a difference of 10° or more between right and left thumbs in extension, and 12% had a difference of at least 15°. In flexion, 22% of thumbs differed by 10° or more and 3% by 15° or more. Comparison with the uninjured contralateral thumb is unreliable in many individuals. We recommend the lack of a definite end point on stress examination as indicating complete rupture of the ulnar collateral ligament.
Radial collateral ligament injuries of the thumb.
Source
New York University-Hospital for Joint Diseases, New York, NY 10003, USA.
Abstract
Radial collateral ligament (RCL) injuries of the thumb are relatively common although they are less common than ulnar collateral ligament injuries, which make up 10% to 42% of collateral ligament injuries of the thumb. The RCL is especially important for pinch movements and for movements of depression. Complete disruption of the RCL can result in both static and dynamic instability, which can lead to a predictable sequence of a painful deformity resulting in articular degeneration. Most authors agree that both acute and chronic grade 3 RCL tears should be surgically treated. There are various methods of repair or reconstruction of the RCL that yield satisfactory results, providing radial stability and intending to preclude the appearance of degenerative disease of the metacarpophalangeal joint. This article reviews the anatomy, physiology, diagnosis, and treatment, including surgical technique, for RCL injuries of the thumb.
additional references: PDF articles
Campbell CS. Gamekeeper's thumb. J Bone Joint Surg Br. Feb 1955;37-B(1):148-9. article in PDF
 copy.jpg "tl_files/pages/home/messenger_code_131702384704 (1) copy.jpg")
