Carpal Boss
Clinical Characteristics
The dorsal wrist ganglion is most often confused with the carpal boss, so named by the French physician Foille. The carpal boss is an osteoarthritic spur that develops at the base of the second and/or third carpometacarpal joints. (figure 1) A firm, bony, nonmobile, tender mass is visible and palpable at the base of the carpometacarpal joints, especially when the wrist is volar flexed.
Radiologically, the mass is best visualized with the hand in 30 to 40 degrees supination and 20 to 30 degrees ulnar deviation ("carpal boss view")( figure 2).Additional imaging such as CT scan or MRI may also be used.
The boss is more common in women (2:1), in the right hand (2:1), and between the third and fourth decades. The mass may be asymptomatic, but the patient may complain of considerable pain and aching. A small ganglion is associated with the carpal boss in 30 percent of cases, adding to its confusion with the more common dorsal wrist ganglion.
Injection to the ganglion or to the cmc joint may be used to reduce pain and irritation. This may be combined with splinting and anti inflammatory medication and avoidance of trauma to the back of the hand\
If symptoms persist at times surgery may be offered. (figure 2) Surgery may involve the removal of the prominent bone, the excision of an associated ganglion or cyst and at times involves tenosynovectomy or tenolysis of adjacent affected tendons. What occurs during surgery may depend upon the preoperative findings as well as the surgical intra operative findings
There can be the persistence of a mass because of excision of the ganglion alone or inadequate excision of the osteophytes. Pain will persist unless all abnormal abutting surfaces have been excised. Dorsal wrist ganglions can present over the carpometacarpal joints and must be distinguished from the carpal boss with its own associated ganglion. Avoidance of injury to branches of the radial and ulnar sensory nerves is again stressed. However the boss can recur and recurrence does not mean that thee intial excision was inadequate. Bone may reform even after proper excsion.
Therapy may be needed after surgery for stiffness or weakness. While not all patients need therapy, all patients should be aware that therapy can be helpful and in those cases where therapy is called for, failure to get therapy in a timely fashion can make postoperative symptoms linger longer or persist.
Recurrence is rare but possible even after proper resection. In some series and reports there is a recurrence rate even after surgery of 5-6%. If there is concern for a recurrence after surgery repeat surgery may be offered and a more wide or extensive resection may be needed. One must differentiate recurrence vs persistant scar or skin tenderness as the tissue may in some be persistantly irritated Therapy is often used to help reduce symptoms before secondary surgery is offered. Sometime recurrence is mangaged with a limited wrist fusion of the involved CMC joints depending upon the extent of the resection needed and the quality, stablity and amount of the remaining joint or joints.
More informaton:
Diagnosis and Treatment of Symptomatic Carpal Bossing
The carpal boss. A 20-year review of operative management
related topic GANGLION CYSTS

figure 1. The carpal boss view is a separate stress view taken in flexion and ulnar deviation with the xray tube angled.
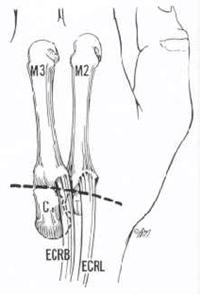
Figure 2. Many surgeons will use a longitudinal extensile incision to expose and treat concurrent pathology
 copy.jpg "tl_files/pages/home/messenger_code_131702384704 (1) copy.jpg")
